

Can tobacco give us a COVID-19 vaccine? Also, why the first vaccine might not be a successful one.
Can tobacco give us a COVID-19 vaccine? Also, why the first vaccine might not be a successful one.
Stay with me for a moment. This is not a crackpot idea from a WhatsApp forward.

Tobacco is the single greatest cause of preventable death in the world, resulting in 5.4 million people killed every year. India has over 100 million smokers and 1 million adult deaths from this deadly habit each year.
Now, tobacco plants might be able to save many lives too.
Two companies, including cigarette giant British American Tobacco, who is the maker of Camel and Dunhill brands of cigarettes, want to grow coronavirus vaccines in fast-growing tobacco plants. Yes, you read that right. We might soon have vaccines made in tobacco plants.

For nearly two decades, certain plants have been genetically-modified to make drugs. Genetically modified (GM) tobacco can make antigens and many different kinds of substances that kill harmful bacteria and viruses. We can also make vaccines, in particular, a certain kind called a virus-like particle (or VLP for short) using GM plant material. It is inexpensive to create a vaccine in plants and can be scaled up, because plants require few resources. They mainly need light and water. Tobacco plants are very well-studied with advanced genetic tools, so they’re a great system for this kind of work.
Here’s how these vaccines are made.
When tobacco plants are a few weeks old they’re dipped in a solution of genetically-altered microorganisms that can naturally infect them. These microorganisms instruct the plants to make proteins that are the key component of the required vaccine. A week after infection, plants are harvested and the protein for the vaccine is extracted.
Do plant vaccines actually work?
Now, I’m going to get to the really cool part. But to I’ll need to switch gears a bit and talk about influenza for a moment instead of coronavirus, SARS-CoV-2, because the first plant vaccine will likely be a flu shot.
Just a few days ago, an exciting report was published in The Lancet highlighting two major studies. These are the first phase III trials of an influenza plant vaccine. Phase III is the late-stage clinical trial that tests the effectiveness and safety of a vaccine in many diverse people. This is the last major hurdle in the drug and vaccine approval process.
The first study had over 10,000 participants. The vaccine prevented respiratory illness in about a third of people who took it. This didn’t meet the 70% threshold that the study had set. But influenza vaccines are seldom highly effective. In comparison, the commercial influenza vaccine for the same season had only been 15% effective.
The second study, which enrolled over 12,000 people, compared the plant vaccine to a standard influenza vaccine produced in a chicken egg. The plant vaccine was similar in effectiveness to the standard vaccine.
Some people might be concerned with the use of GM plants to create a vaccine. However, up until now there have been no major adverse effects in people. In fact, for influenza, it may actually be the case that genetically engineered vaccines work better than common, cell-derived vaccines. I won’t get into the technical details of why that’s the case but it’s being investigated further.
So far, there’s only been one plant-derived drug for a human disease (for Gaucher's disease), but this is a landmark study because it is the first time that a plant vaccine has gone through clinical trials in people. The field has moved rapidly in just thirty years- from showing that proteins from a virus could be created in plants to an actual vaccine that seems to work. Exciting days are ahead.
How plant vaccines can help fight COVID-19
Although there are many different types of candidate vaccines in different stages of human and animal trials for COVID-19, we don’t know which ones will work best in various populations yet. We also have no idea how to distribute these many vaccines at scale. Production constraints and hoarding by relatively rich countries might limit the supplies of a rare commodity like a vaccine.
During a pandemic it is important to have many different ways to make a vaccine. For example, many of the most deadly influenza strains originate in birds. Having a vaccine platform that doesn’t rely on hens or eggs might help us to circumvent the problem of birds getting sick themselves.
Taking a leaf from their influenza vaccines, Medicago, one of the two companies that is funding research on plant vaccines, is conducting trials with plant vaccine for COVID-19. They’re also working on vaccines for rotavirus and norovirus diseases.
Plant vaccines are not going to overtake traditional vaccines anytime soon for influenza or COVID-19 as the main source of vaccines. But as the current pandemic has shown- we will need many different platforms and resources to immunize billions of people.
What actually is a successful SARS-CoV-2 vaccine?
I asked a question on Twitter a few weeks ago that I feel I should revisit.
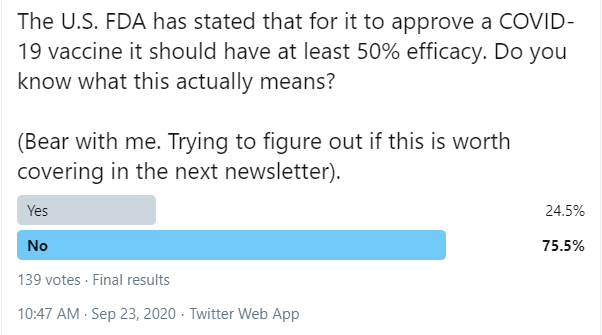
Writing in The New York Times, Carl Zimmer had this to say:
The first vaccines may provide only moderate protection, low enough to make it prudent to keep wearing a mask. By next spring or summer, there may be several of these so-so vaccines, without a clear sense of how to choose from among them. Because of this array of options, makers of a superior vaccine in early stages of development may struggle to finish clinical testing.
One of the crucial questions around COVID-19 vaccines is this: how well will they work? But it’s not a simple question to answer because there are many pieces to the puzzle.
The U.S. Food and Drug Administration has said that a vaccine has to be at least 50% effective for it to be approved for use in the United States. Dr. Anthony Fauci, head of the U.S. National Institute of Health and Infectious Disease would like it to be 75% effective. .
But effectiveness actually can mean very different things based on the “endpoints” that are selected as criteria for success.
One scientist said gone on record to say vaccine effectiveness is related to how effective the vaccine is in preventing disease. Another has said that an effective vaccine results in a decrease in the severity of disease.
The difficultly stems from the situation with SARS-CoV-2.
Not everyone who is infected with SARS-CoV-2 will have symptomatic COVID-19.
Not everyone who has symptomatic COVID-19 will have serious symptoms.
COVID-19 is a biphasic disease. In the first phase, there may be few or no symptoms at all. The second phase seems to harm the elderly and the vulnerable more.
An ideal vaccine will be able to prevent infection altogether. There are indications that some of the vaccines in trials may not be that effective. In such a scenario, we would want few people to have symptoms of serious disease. Six of the leading vaccines contenders have reducing disease severity by 50% as the primary endpoint for success.
In fact, the FDA accepts either prevention of SARS-CoV-2 infection or severe SARS-CoV-2 infection as endpoints for evaluating the success of a vaccine. But both are not the same thing. This was pointed out by superstar German virologist Dr. Christian Drosten in an interview he gave to Die Zeit. The interview is very revealing and I’ve included an excerpt below:
ZEIT ONLINE: Many experts believe that the first-generation vaccines are unlikely to protect against infection. Do you agree?
Drosten: They are more likely to protect against a severe form of the disease than against the infection itself. However, data from experiments with primates also suggests that vaccination reduces the viral load in the throat (for example: New England Journal of Medicine: Corbett et al., 2020). So, I doubt that the virus will spread unhindered under the cover of the vaccination. I also expect that the not-so-great first-generation vaccines will play their part in helping to control the pandemic. If you have enough of them…
… We will have different vaccines, which may even have differing efficacy, and parts of the population will be vaccinated with them. At the same time, contact restrictions and the basic hygiene rules will still be important.
ZEIT ONLINE: Do you have the feeling that this information has already been sufficiently communicated?
Drosten: No, my feeling is that this information hasn’t been conveyed yet. That includes telling people that the vaccines may not be perfect. It could be that they don’t provide sufficient protection or that there are side effects that stand in the way of recommending them for younger people, who tend not to fall seriously ill. I think we need to start preparing people now for a vaccine that may not be perfect. The time has now arrived. It would have been premature earlier because the Phase III trials are only just starting.
Dispelling a myth regarding the Spanish Flu

The descendants of the 1918 virus remain today; as endemic influenza viruses, they cause significant mortality each year.
That doesn’t mean the H1N1 pandemic of 1918-1919 never ended. Of course, it did. It just means that significant numbers of people had already been infected so that when the virus mutated or gave up some of it’s nucleic acid genetic component to other influenza viruses, they were not completely susceptible anymore. Dr. Jeffery Taubenberger who is an expert on the genetics of the 1918 H1N1 strain is the source of this information.
That it for this week…
The link for the hardcover “COVID-19: Separating Fact from Fiction” is now available on Amazon’s Indian site.
Sign up for my newsletter to get weekly issues delivered straight to your inbox.
In previous issues I’ve covered why SARS-CoV-2 is never going to be eradicated, whether wearing glasses reduces the chance of SARS-CoV-2 infection, and what role genetics plays in susceptibility.
I’ve also done detailed newsletters covering the natural history of life, and the weight of all life on the planet.
Future newsletters will cover other important scientific questions: Did scientists actually discover life on Venus? What might life on another planet look like? Why do we consider birds living dinosaurs? What’s the connection between sharks and COVID-19?